
International Journal of Clinical and Medical Research
ISSN Print: N/A
ISSN Online: 3134-8831
About: International Journal of Clinical and Medical Research (IJCAMR) is an open-access, peer-reviewed journal dedicated to the publication of high-quality research in the field of clinical and medical sciences. The journal aims to provide a platform for researchers, clinicians, and healthcare professionals to share knowledge, exchange ideas, and promote scientific advancement in healthcare.
International Journal of Clinical and Medical Research | Year 2025 | Volume 2 | Issue 2 | Pages 35-36
Spontaneous Pneumothorax in Severe COVID-19: A Case Report with Literature Review
Fahmida Khatoon 1*1Department of Biochemistry, College OF Medicine, University OF Ha’il, Saudi Arabia
2Department of Nursing, College of Nursing and Health Sciences, Jazan University, Saudi Arabia
3College of Medicine, University of Hail, Hail, Saudi Arabia
View PDF Download XML Download DOI XML DOI: 10.66590/ijcmr2025020205
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first identified in late 2019 in Wuhan, China, rapidly evolved into a global health crisis. Pneumothorax is an uncommon complication of coronavirus disease 2019 (COVID-19), reported in approximately 1–2% of cases, while pneumomediastinum is even less frequent. Case Presentation and Discussion: Pneumothorax associated with COVID-19 is most often observed in patients with severe disease, particularly those requiring mechanical ventilation. Elevated positive end-expiratory pressures and reduced lung compliance, often related to fibrotic changes, may predispose these patients to alveolar rupture. However, cases have also been documented in patients receiving non-invasive support or even without oxygen therapy, suggesting that SARS-CoV-2 infection itself may independently increase the risk of pneumothorax. Clinicians should therefore consider this complication in any patient presenting with sudden respiratory deterioration. Management generally follows standard pneumothorax treatment protocols. However, procedures such as chest tube insertion may pose an increased risk of aerosol generation and viral transmission, necessitating strict infection control precautions. Conclusion: This report describes a case of pneumothorax in a non-smoking patient admitted to intensive care for severe COVID-19. The case underscores the importance of early recognition of this rare but potentially serious complication and highlights considerations for safe clinical management.
INTRODUCTION
SARS-CoV-2 was first identified at the end of 2019, in the Wuhan region (China), subsequently spreading worldwide with a major impact on health and economic system [1]. A pneumothorax is a rare complication, affecting between 1–2% of SARS-CoV-2 cases. Pneumomediastinum is even rarer [2] we report the case of a pneumothorax occurring in a non-smoking patient hospitalized in intensive care for treatment of a serious SARS COV 2.
Observation
Our patient is 66-year-old no smoker, with no particular medical or surgical history. He had consult in the emergency room for a respiratory distress with no fever one week after an influenza-like illness treated as SARS cov 2 because of a positive PCR test.
The clinical examination finds an agitated patient, hypoxic at 55% saturation, polypnea at 40 cycles per minute, with signs of struggle and tachycardia at 120 beats per minute with a blood pressure at 165 mmHg systolic and 100 mmHg of diastolic. The chest X-ray and the pleural ultrasound did not show any signs in favor of pneumothorax.
The treatment consisted on admission to intensive care unit, the use of non-invasive ventilation in the prone position alternating with the high-concentration mask at 15 liters per minute.
introduction of empiric antibiotic therapy based on cephalosporin and ciprofloxacin with corticosteroid therapy and platelet antiaggregation associated with curative anticoagulation because inflammatory markers and D-dimers were high.
The evolution was initially good with a decrease in oxygen requirements and improvement in gasometer results.
A relapse with re-aggravation of our patient's condition was noticed during the third day of his stay in intensive care unit, a chest CT scan (Figure 1) was performed showing diffuse bilateral ground glass lesions related to infectious pneumopathy type Covid -19 with anterior left pneumothorax of low abundance.
The patient was intubated after managing of the pneumothorax by using a thoracic drainage; introduction of a nosocomial antibiotic therapy based on carbapenem and amikacine in front of the installation of a hemodynamic instability, reason why elevated dose of vaso-actif drugs have been used. The patient subsequently presented alveolar hemorrhage and then died after 2 days.
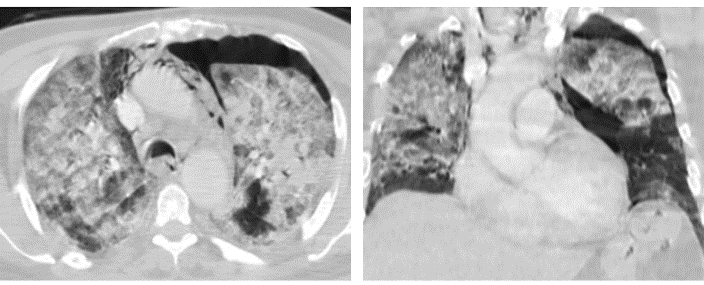
Figure 1: Thoracic CT Scan in Axial and Coronal Section (Parenchymal Window) Showing Diffuse Bilateral Ground Glass Lesions Related to Infectious Pneumopathy Type Covid-19 with Anterior Left Pneumothorax of Low Abundance
DISCUSSION
SARS-CoV-2 was first identified at the end of 2019, in the Wuhan region (China), subsequently spreading worldwide with a major impact on health and economic system [1].
All organs can be affected but the main complications are severe pneumonia, Acute Respiratory Distress Syndrome (ARDS), heart damage, liver damage which can lead to acute hepatocellular insufficiency and kidney damage [3].
A pneumothorax is a rare complication, affecting between 1–2% of SARS-CoV-2 cases. Pneumomediastinum is even rarer [2].
Pneumothorax in the context of SARS-CoV-2 infection mainly occurs in patients with a severe form of the infection and requiring mechanical ventilation. This type of ventilation makes it possible to impose high positive expiratory pressures which can be complicated by pneumothorax when patients present with a lack of compliance secondary to fibrosis. Nevertheless, cases under conventional ventilation including without oxygen therapy are possible, suggesting that SARS-CoV-2 infection could be an independent risk factor for pneumothorax. Therefore, any worsening of the respiratory picture should evoke a pneumothorax [4].
The hypothesis of the destruction of the lung parenchyma by SARS-CoV-2 and the formation of a cyst as a mechanism leading to pneumothorax is all the more probable since these lesions are occasionally described in the radiological evolution of the disease [5].
The management of pneumothorax secondary to SARS-CoV-2 pneumonia is usual. Placement of a chest drain could increase the risk of aerosol dissemination. The operator must therefore equip himself accordingly and secure the drainage system according to the recommendations in force. The management of a pneumo-mediastinum is symptomatic as long as no sign of severity, such as mediastinal compression, is observed [6-8].
CONCLUSIONS
Despite pneumothorax in this clnical scenario represents a frequent complication, only few papers focused on imaging find- ings related to mechanical ventilation complications in Covid-19 patients have been reported.
Any worsening of the respiratory situation should suggest a pneumothorax. Imaging techniques are key in the diagnosis and management of these complications.
REFERENCES
- “Coronavirus disease (COVID-19).” World Health Organization, https://www.who.int/fr/emergencies/ diseases/novel-coronavirus-2019/question-and-answers -hub/q-a-detail/coronavirus-disease-covid-19.
- Chen, N., et al. “Epidemiological and clinical characteristics of 99 Cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study.” Lancet, vol. 395, 2020, pp. 507–513.
- Yang, F., et al. “Analysis of 92 deceased patients with COVID-19.” J Med Virol, vol. 92, 2020, pp. 2511–2515.
- Pierre, L., et al. “Pneumothorax et SARS-CoV-2: Analyse rétrospective de 18 Cas.” Infectious Diseases Now, vol. 51, 2021, pp. S56–S74.
- Liu, J., et al. “Clinical and radiological changes of hospitalised patients with COVID-19 pneumonia from disease onset to acute exacerbation: A multicentre paired cohort study.” Eur Radiol, vol. 30, 2020, pp. 5702–5708.
- Ferreira, J.G., et al. “Pneumothorax as a Late Complication of COVID-19.” Rev Inst Med Trop Sao Paulo, vol. 62, 2020, p. e61.
- Pieracci, F.M., et al. “Tube thoracostomy during the COVID-19 pandemic: Guidance and recommendations from the AAST acute care surgery and critical care committees.” Trauma Surg Acute Care Open, vol. 5, 2020, pp. e000498.
- Shan, S., et al. “Spontaneous pneumomediastinum, pneumothorax and subcutaneous emphysema in COVID-19: case report and literature review.” Rev Inst Med Trop Sao Paulo, vol. 62, 2020, pp. e76.