
International Journal of Clinical and Medical Research
ISSN Print: N/A
ISSN Online: 3134-8831
About: International Journal of Clinical and Medical Research (IJCAMR) is an open-access, peer-reviewed journal dedicated to the publication of high-quality research in the field of clinical and medical sciences. The journal aims to provide a platform for researchers, clinicians, and healthcare professionals to share knowledge, exchange ideas, and promote scientific advancement in healthcare.
International Journal of Clinical and Medical Research | Year 2025 | Volume 2 | Issue 2 | Pages 30-34
Diagnostic Utility of High-Resolution Thoracic Ultrasound in Pleural Effusion: A Prospective Study from Tikrit
tes test 1* , Usama Nahi Hamdi2, Salah Mohi Salih3, Maysaloon Ahmed Khudhair4 and Sarab K. Abedalrahman 5*1test
2M.B.Ch. DMRD, MSC Rad, EFBR, Salahdeen General Hospital-Salahdeen Health Directorate, Iraq
3M.B.Ch. DMRD, MSc Rad Salahdeen General Hospital- Cancer Management Specialty Center, Salahdeen Health Directorate, Iraq
4College of Medicine-Tikrit University, Iraq
5Consultant Cancer Screening, Cancer Screening Subspecialty, Cancer Management Specialty Center, Salahdeen Health Directorate, Iraq
View PDF Download XML Download DOI XML DOI: 10.66590/ijcmr2025020204
Abstract
Background: Accurate evaluation of pleural effusion is crucial for effective clinical management. This study aimed to compare the diagnostic value of high-resolution thoracic ultrasound with chest radiography in patients presenting with pleural effusion. Methods: A prospective observational study was conducted in the Radiology Department of Salah Al-Deen General Hospital from April 2022 to February 2023. A total of 23 patients diagnosed with pleural effusion were included, comprising 13 males and 10 females, with a mean age of 49 years (range: 14–74 years). All participants underwent detailed clinical, laboratory and radiological assessments. The diagnostic performance of thoracic ultrasound was compared with chest radiography in terms of accuracy and characterization of pleural effusion. Results: A statistically significant difference was observed between chest radiography and ultrasound in the evaluation of pleural effusion (p<0.001). Thoracic ultrasound demonstrated superior accuracy in assessing both the nature and extent of pleural effusion. The sensitivity of ultrasound was 78%, whereas chest radiography showed limited reliability, particularly in estimating the volume of effusion. Moreover, ultrasound was more effective in differentiating types of pleural effusion and detecting loculated collections. Conclusion: High-resolution thoracic ultrasound is a reliable, non-invasive and bedside imaging modality with greater diagnostic accuracy than chest radiography for evaluating pleural effusion. It also plays a pivotal role in guiding thoracentesis, ensuring safe chest tube placement and monitoring fluid drainage, especially in critically ill or mechanically ventilated patients.
INTRODUCTION
- The pleural cavity is a potential space between the visceral and parietal pleurae. The parietal pleura lines the chest wall, while the visceral pleura covers the lungs, including associated blood vessels, bronchi and nerves. Under normal conditions, a thin layer of fluid (approximately 5–15 mL) is present within this space, serving as a lubricant to facilitate smooth respiratory movements [1]
- Pleural effusion occurs when there is an abnormal accumulation of fluid within the pleural cavity due to various pathophysiological mechanisms. These include increased pulmonary capillary pressure, enhanced pleural membrane permeability, reduced oncotic pressure and obstruction of lymphatic drainage [2–4]. Based on its pathogenesis, pleural effusion is broadly classified into Transudative Pleural Effusion (TPE) and Exudative Pleural Effusion (EPE). Exudative effusions are typically associated with pathological conditions affecting the pleura, such as malignancy and tuberculosis [5,6], whereas transudative effusions are usually caused by systemic conditions like liver cirrhosis and congestive heart failure, which alter fluid formation and absorption [7]
- Diagnostic evaluation of pleural effusion often involves thoracentesis, where pleural fluid is obtained for biochemical analysis [8]. However,
thoracentesis is an invasive procedure and may not be suitable for elderly, critically ill, or bedridden patients [9]. In this context, imaging modalities play a crucial role. Thoracic ultrasonography has demonstrated high sensitivity and accuracy in detecting, localizing and characterizing pleural effusions. It is widely favored due to its non-invasive nature, safety, ease of use and high patient acceptance [10]
- Despite these advantages, there remains limited evidence regarding the reliability of specific Thoracic Ultrasonography (TUS) findings in differentiating types of pleural effusion. Therefore, this study aims to evaluate the clinical applications and diagnostic performance of high-resolution thoracic ultrasound in the assessment of pleural effusion and to compare its diagnostic accuracy with chest radiography
MATERIAL AND METHODS
This prospective observational case-series study was conducted in the Radiology Department of Salah Al-Deen General Hospital from April 2022 to February 2023. A total of 23 patients presenting with respiratory complaints were included. The age of participants ranged from 14 to 80 years.
All patients underwent a comprehensive evaluation, including detailed history taking, clinical examination, chest radiography (CXR) and thoracic ultrasonography. Chest X-rays were performed in erect posteroanterior and lateral views using a Shimadzu Corporation X-ray system. Thoracic ultrasound examinations were carried out using a GE Healthcare LOGIQ 9 ultrasound machine equipped with a 3.5–5 MHz convex transducer.
The diagnostic accuracy of ultrasound was assessed by comparing its findings with chest radiography and the final diagnosis, which was established based on clinical outcomes, operative findings and histopathological examination results. Data analysis was performed using IBM SPSS Statistics (Version 21).
Ultrasound Technique
Two types of transducers were utilized:
- A 3.5–5 MHz convex transducer, which was primarily used for pleural imaging due to its adequate penetration and field of view
- A 7.5–10 MHz linear transducer, applied when higher-resolution imaging was required for detailed assessment of pleural abnormalities.
Scanning Procedure
Thoracic ultrasound was performed using gray-scale, real-time imaging. Dynamic noise filters were avoided to prevent interference with the visualization of lung sliding.
The transducer was positioned perpendicular to the skin surface, with the marker oriented cephalad and scanning was performed through the intercostal spaces. Patients were examined in a seated position whenever possible. Each hemithorax was systematically evaluated and divided into anterior, lateral and posterior zones, demarcated by the anterior and posterior axillary lines. A longitudinal probe orientation along the parasternal line was used for optimal visualization.
RESULTS
The age of participants ranged from 14 to 74 years, with a mean age of 49.2±17.6 years and a median age of 55 years. The most frequent age groups were 50–59 and 60–69 years, with 55 years representing the 50th percentile.
A total of 13 participants (56.5%) were male. Notably, all participants above the age of 40 years were male. The distribution of pathological findings showed that neoplastic conditions occurred equally in both sexes (4 cases each), whereas reactive and inflammatory conditions were more common among males compared to females (17% vs. 4%).
Regarding the distribution of pleural effusion (PE), the majority of cases were right-sided. Specifically, 43.5% of cases were confined to the right side, while 30.4% were confined to the left side. Bilateral effusion was observed in some cases, with 17.4% being predominantly right-sided and 8.7% predominantly left-sided. The sidedness of pleural effusion showed good correlation between ultrasonography and chest radiography findings.
Histopathological examination of pleural fluid obtained via ultrasound-guided thoracentesis revealed that most cases were exudative in nature (69.6%), while transudative effusions accounted for 30.4% of cases. Analysis of etiological factors indicated that hypoproteinemia and reactive transudative effusions were significantly more common in patients older than 40 years (p<0.05). However, no statistically significant association was found between specific etiologies and exudative effusion, as these cases were distributed across all age groups.
Final diagnoses for each case were established through a combination of clinical evaluation, radiological findings (including adjunct imaging such as CT or MRI when required) and pleural fluid analysis. The distribution of diagnoses is presented in Figure 1.
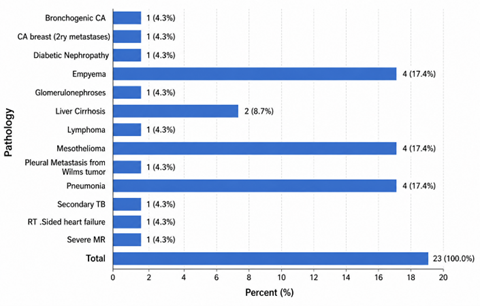
Figure 1: Frequency of Pathologies Among the Study
Pathological Criteria in US
All cases underwent thoracic ultrasound examination of the pleural cavity using the previously described technique. Sonographic assessment included evaluation of echogenicity, presence or absence of septations, fluid volume and detection of any associated mass lesions. Based on these findings, each case was classified according to its sonographic diagnosis.
Statistical analysis using the Chi-square test demonstrated that exudative pleural effusions were significantly associated with moderate to large fluid volumes, whereas transudative effusions were typically minimal to moderate in volume (p<0.05). The presence of turbid fluid was strongly associated with exudative effusions, particularly in cases of empyema (p = 0.03). However, fluid volume alone was not a reliable distinguishing factor (p = 0.001).
Mass lesions were predominantly observed in neoplastic conditions, showing a significant association (p = 0.001), although the absence of a mass did not exclude malignancy (p≥0.05). Regression analysis revealed that none of the evaluated sonographic parameters independently predicted the final histopathological diagnosis with high certainty, with coefficient of determination (R²) values ranging from 17% to 50%.
Septations were detected in 26% of cases, while 74% showed no septations on ultrasound examination. Fluid echogenicity proved to be a strong indicator in differentiating between exudative and transudative pleural effusions, with a highly significant association (p = 0.001). However, echogenicity was not significantly correlated with the specific underlying etiology (p≥0.05).
Regarding chest radiography, 47% of cases were considered conclusive in identifying or suggesting the underlying pathology, whereas 52% required further radiological evaluation. Chest X-rays provided additional information on associated findings such as lung collapse, mediastinal shift and cardiac silhouette changes. In contrast, thoracic ultrasonography was more focused on pleural pathology. Therefore, both imaging modalities demonstrated complementary rather than mutually exclusive roles in the evaluation of pleural effusion.
Pleural US Diagnosis Outcome
Regarding outcome studies, sensitivity and specificity were measured despite low volume sample. The sensitivity and specificity were (83.0%, 60%) respectively. The positive predictive value and negative predictive value were (88.2%, 50%) respectively. The degree of accuracy of US to diagnose the PE first into transudative or exudative and second into subcategorizing the effusion into malignant or inflammatory was 78.5% (Figure 1,2).

Figure 2: Pleural Effusion Due to Sever MR and ASD: 46 years old Male Complained of Central Chest Pain of 2 Weeks Duration: X-Ray Reveled Globular Cardiac Shape and Enlarged in Size, with Opacity at Right Lower and Middle Lope of Lung and Obliteration of Costophrenic Recesses Ultrasound Examination Revealed Right Sided Mild Pleural Effusion, Clear Fluid, No Pleural Thickening, No Mass
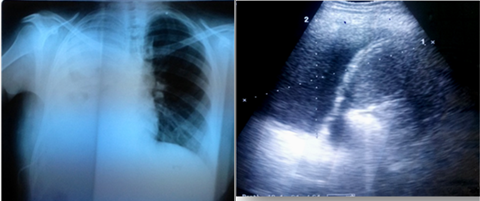
Figure 3: Lung Metastasis Secondary to ca. Breast. A 27 Years Old Female Complained of Shortness of Breath for 3 Months: X-Ray Reveled Diffuse Right Sided Lung Opacity, Left Side Peri-Hialer Nodular Opacities, No Shifting of Mediastinal Structure to Opposite Side. Ultrasound Examination Revealed Sever Right Sided Pleural Effusion, Clear Fluid, No Septation or Mass is Seen, US Guiding Aspiration and Pleurodesis Was Done
DISCUSSION
The present study revealed that age ranged from (14-74y) with mean of (49.2+/-17.6). The median age was 55y and the most frequent categories were 50-59 & 60-69. The 55year was the 50th. Also it revealed that most of cases were of exudative nature (69.565%) versus transudate (30.435%). This agree with Entsar S. in 2017 found that the male patients formed 56% (47 patients), whereas female patients constituted 44% (37 cases); their mean age was 51.21±14.1 years (range:14–80 years). Seventy-three (86.9%) cases had exudative effusions; inflammatory causes (n = 33) and malignancy (n = 31) were the most common [11]. Our study agrees with Wang T in 2022 found that some sonographic features of pleural effusion, such as echogenicity, septation and pleural thickening, had a high frequency of appearance in exudative pleural effusion. Among the common diseases leading to exudates, empyema has the highest proportion of positive findings on ultrasonographic imaging [12]. Sajadieh H in 2004, Asciak R in 2019, Huang J 2018 found that ultrasonography was considered an alternative to aspiration in determining the nature of pleural effusion, especially in older individuals. In their results, anechoic effusion was observed in 100% transudates and 14% exudates [13-15]. However, Shkolnik B in 2020 found that the TUS findings of 300 consecutive pleural effusions and found that an anechoic appearance was associated with 56% of exudative effusions compared to 44% of transudative effusions. Complex-appearing effusion, which had a positive value of 90%, was a high predictor of exudation effusion [16].
The present study goes with Yang et al in 2017 analyzed sonographic images of 320 patients with pleural effusion and showed that all patients with transudates presented anechoic appearance on ultrasonography (96/96), whereas anechoic effusion could be a transudative pleural effusion or exudative pleural effusion (33.9%). Moreover, internal echogenicity of complex patterns and pleural thickening tended to occur in exudative pleural effusion [17]. Amr A in 2021 Menoufia experience found that the type of pleural effusion was exudate (75.8%) versus (24.2%) of cases was transudate. And the total of 37 (52.9%) patients were males and 33 (47.1%) were females. The mean age of the patients was 54.8±11.8 years. Transudate pleural effusion was anechoic 11 (64.7%) versus 0 (0%) in exudate pleural effusion. Echogenic found in transudate pleural effusion 6 (35.3%), versus 19 (35.8%) in exudate pleural effusion. The complex nonseptated 21 (39.7%) versus complex septated 13 (24.5%) in exudate pleural effusion, while 0 (0%) in transudate pleural effusion.
Effusion size was small 3 (17.6%), moderate 11 (64.8%), massive 3 (17.6%) in transudate pleural effusion, versus small 9 (17%), moderate 34 (64.2%), massive 10 (18.8%) in exudate pleural effusion. Septation was positive in 13 (24.5%) of patients with exudate pleural effusion versus 0 (0%) transudate pleural effusion. Septation was negative 17 (100%) of patients with transudate pleural effusion versus 39 (73.6%) of patients with exudate pleural effusion. The side of the pleural effusion was unilateral 53 (100%) of patients with exudate pleural effusion versus transudate pleural effusion 0 (0%) of cases. The side of the pleural effusion was bilateral in 17 (100%) of patients with transudate pleural effusion versus exudate pleural effusion in 0(0%) of cases [18].
Bhutta MR in 2023, studied a total of eighty patients were involved in the research that underwent USG and CT within 72 hours and found that the pleural effusion could be caused by multiple factors, including congestive heart failure 8 (10.0%), malignant infections 15 (18.8%), acute pulmonary embolism 3 (3.8%), chronic kidney disease 4 (5.0%), liver cirrhosis 4 (5.0%) and other diseases like dengue or typhoid 10 (12.5%).
Also they found that 51/80 (63.75%) of the patients had exudate pleural effusion versus 29/80 (36.25%) transudate pleural effusion. Echogenic found in 5 (17.2%) transudate pleural effusion versus 14 (27.5%) exudate pleural effusion. Moderate to large effusion size was noted in Exudates pleural effusion, while transudate had a smaller effusion size in most cases. Transudative effusions were frequently seen bilaterally 22 (75.9%). On the other hand, exudative effusions were frequently seen unilaterally 49 (83.1%) with a significant p-value of less than 0.01. The PE were unilateral 7 (24.1%) in transudate versus exudate 49 (96.0%) of the cases (p<0.01). While PE were bilateral 22 (75.8%) in transudate versus exudate 2 (4.0%) <0.01, this means that exudative effusions mainly unilateral, while transudate effusions mainly bilateral [19]. Regarding echogenicity, similar results found by Bhutta MR in 2023 and Jaworska et al in 2020, as stated by Jaworska et al. signs like thickened pleura and variation in lung parenchymal tissue were also important indicators of exudative fluid [19,20]. Kumari, Jaseemudheen in 2023 found that ultrasound is a feasible imaging modality for diagnosing pleural effusion because there is no radiation involved. Also, it is the safest modality for pleural fluid drainage and biopsy as it provides real-time imaging with better efficacy and more safety to patients [21].
The current study results regarding sensitivity and specificity and the positive predictive value and negative predictive value goes in agreement with ElShaimaa M. Mohamed in 2018, the sensitivity, specificity and diagnostic accuracy of bedside CXR were 76.2, 70.6 and 75% for pleural effusion versus 100%, 100% and 100% for pleural effusion, respectively [22]. Also agree with Entsar S in 2017, found that US is better than CT in the detection of pleural effusion, as US detected all (84/84) cases of effusion, even the small subpulmonic effusion, whereas CT detected 98.8% (83/84) of cases and missed one case [11]. Also agree with Helala LA in 2015 who reported that US (49/50) was better compared with CT (45/50) in the detection of pleural effusion in critically ill ICU patients [23]. Moreover, these results are in agreement with the study by Abu-Youssef et al., who reported that US and CT were well correlated in the detection of pleural effusion [24].
CONCLUSIONS
Thoracic ultrasound demonstrated a sensitivity of 78% in detecting pleural effusion, whereas chest radiography was less conclusive, particularly in accurately estimating the volume of pleural effusion. These findings highlight the superiority of ultrasound over radiography in the evaluation of pleural fluid.
Thoracic ultrasonography is a simple, non-invasive bedside imaging modality with higher sensitivity and specificity compared to chest radiography for the diagnosis of pleural effusion. In addition to detection, it plays a crucial role in differentiating between various types of pleural effusions based on their sonographic characteristics.
Moreover, ultrasound guidance has been increasingly recommended for invasive procedures such as thoracentesis and chest tube insertion, as it enhances procedural safety and accuracy. This is especially important in critically ill or mechanically ventilated patients, as well as in cases of small or loculated effusions.
Furthermore, thoracic ultrasound is valuable for real-time monitoring of pleural fluid drainage, enabling clinicians to assess treatment response and determine the appropriate timing for removal of drainage devices.
REFERENCES
- Charalampidis, C., et al. “Pleura space anatomy.” Thorac Dis, vol. 7, suppl. 1, 2015, pp. S27–S32.
- McGrath, E.E. and P.B. Anderson. “Diagnosis of pleural effusion: A systematic approach.” Am J Crit Care, vol. 20, 2011, pp. 119–127.
- Ferreiro, L., et al. “Advances in Pleural Effusion Diagnostics.” Expert Rev Respir Med, vol. 14, 2020, pp. 51–66.
- Allama, A.M., et al. “Pleural and Serum Markers for Diagnosis of Malignant Pleural Effusion.” Asian Cardiovasc Thorac Ann, vol. 28, 2020, pp. 560–565.
- Bielsa, S., et al. “Tuberculous Pleural Effusion: Clinical Characteristics of 320 Patients.” Arch Bronconeumol (Engl Ed), vol. 55, 2019, pp. 17–22.
- Ferreiro, L., et al. “Management of pleural infections.” Expert Rev Respir Med, vol. 12, 2018, pp. 521–535.
- Cartin-Ceba, R. and M.J. Krowka. “Pulmonary complications of portal hypertension.” Clin Liver Dis, vol. 23, 2019, pp. 683–711.
- Cornes, M.P., et al. “The impact of between analytical platform variability on the classification of pleural effusions into exudate or transudate using light’s criteria.” J Clin Pathol, vol. 70, 2017, pp. 607–609.
- Ferreiro, L., et al. “Diagnosis and management of pleural transudates.” Arch Bronconeumol, vol. 53, 2017, pp. 629–636.
- Hansell, L., et al. “Lung ultrasound has greater accuracy than conventional respiratory assessment tools for the diagnosis of pleural effusion, lung consolidation and collapse: A systematic review.” J Physiother, vol. 67, 2021, pp. 41–48.
- Ahmeda, E.S., et al. “Role of Ultrasonography in the Diagnosis of Pleural Effusion.” Egypt J Bronchol, vol. 11, 2017, pp. 120–127.
- Wang, T., et al. “Value of ultrasonography in determining the nature of pleural effusion: Analysis of 582 cases.” Medicine (Baltimore), vol. 101, no. 33, 2022, pp. e30119.
- Sajadieh, H., et al. “Ultrasound as an alternative to aspiration for determining the nature of pleural effusion, especially in older people.” Ann NY Acad Sci, vol. 1019, 2004, pp. 585–592.
- Asciak, R., et al. “Prospective Analysis of the Predictive Value of Sonographic Pleural Fluid Echogenicity for the Diagnosis of Exudative Effusion.” Respiration, vol. 97, 2019, pp. 451–456.
- Huang, J., et al. “Thoracic ultrasound versus artificial pneumothorax in complications of medical thoracoscopy a propensity score matching analysis.” J Thorac Dis, vol. 10, 2018, pp. 5269–5274.
- Shkolnik, B., et al. “Diagnostic accuracy of thoracic ultrasonography to differentiate transudative from exudative pleural effusion.” Chest, vol. 158, 2020, pp. 692–697.
- Yang, W., et al. “Infectious pleural effusion status and treatment progress.” J Thorac Dis, vol. 9, 2017, pp. 4690–4699.
- Drawisha, A.A., et al. “Chest ultrasonography versus computed tomography in the diagnosis of pleural effusion (Menoufia Experience).” The Egyptian Journal of Chest Diseases and Tuberculosis, vol. 70, 2021, pp. 395–402.
- Bhutta, M.R., et al. “Diagnostic accuracy of ultrasound and computed tomography in differentiating transudate from exudate in patients with pleural effusion.” Pak Armed Forces Med J, vol. 73, no. 2, 2023, pp. 473–476.
- Jaworska, J., et al. “Consensus on the application of lung ultrasound in pneumonia and bronchiolitis in children.” Diagnostics (Basel), vol. 10, no. 11, 2020, pp. 935.
- Kumari, S. and M.M. Jaseemudheen. “Assessment of pleural effusion by means of imaging modalities.” Journal of Health and Allied Sciences, vol. 13, no. 3, 2023, pp. 301–305.
- Mohamed, E.M. “In Diagnosis of pleural effusion and pneumothorax in the intensive care unit patients: Can chest US replace bedside plain radiography?” The Egyptian Journal of Radiology and Nuclear Medicine, vol. 49, no. 2, 2018, pp. 346–351.
- Helala, L.A., et al. “Role of ultrasound in diagnosis and treatment of pleural diseases in respiratory intensive care unit.” Egypt J Bronchol, vol. 9, 2015, pp. 79–79.
- Abu-Youssef, H., et al. “Study of the added value of transthoracic ultrasound in staging of lung cancer.” Egypt J Chest Dis Tuberc, vol. 63, 2014, pp. 1025–1034.